
Dear Friends,
Sorry I have been gone for 3 weeks. As soon as I arrived home from Japan I came down with COVID, and I've been sick for 2 weeks and as you may recall, the brain does not function normally during this biological warfare agent infection.
I'm nearly over it and have managed to write two articles that I had been wanting to cover. Both are included below.
The first is about the self-amplifying mRNA COVID vaccine that was just rolled out in Japan. The bottom line is that by harnessing your cellular machinery to make many copies of both messenger RNA and spike protein, you need a lot less vaccine material for the same antibody response, so it is cheaper and quicker to make this vaccine than earlier mRNA vaccines.
It is supposed to last longer in your body, making mRNA and spike protein potentially forever. I cannot predict its duration or effect nor negative effects because I have not seen or heard any data on this.
It is remarkable that a vaccine being touted for its longer duration of effect has had released no data regarding how long it actually keeps working.
Japanese doctors are very concerned that the vaccine itself may spread between people. It is important to note that FDA is also concerned about gene therapy products spreading to other people: it asked manufacturers of gene therapies to study whether they will spread (shed) in its gene therapy guidance document.
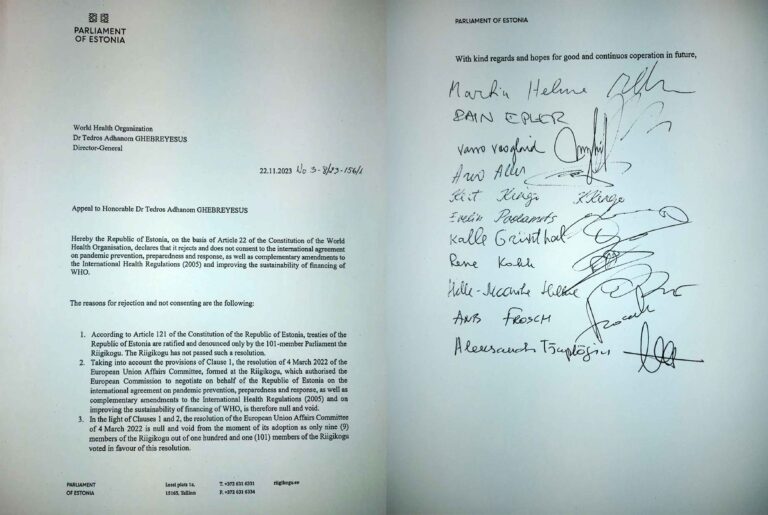
The Japanese doctors are wisely saying look, if you can't show us this stuff doesn't spread, or isn't dangerous, you shouldn't be licensing it or allowing it to be used. Their message has gotten out, and we at the International COVID Summit 6 were there to support them.
Below is my article about the self-amplifying vaccines.
Below that is an article about the many new organizations that have sprung up to push the pandemic preparedness agenda and garner money for it. Hope you enjoy them.
Sincerely yours,
Meryl
Self-amplifying mRNA vaccines
2 gutsy companies (Arcturus and CSL) test drive their first-in-class vaccine in Japan–and how this ties in with the 100 day vaccine promise of CEPI and the globalists

Bottom line: there are no long-term data on these vaccines. And since they might produce the spike protein, an indisputably dangerous toxin, indefinitely, it would be crazy to use this vaccine. But since the era of COVID began, the precautionary principle was thrown out, and the more risks a vaccine manufacturer and regulator take, the better, it seems.
Here is what the manufacturer Arcturus claims as the benefits of this vaccine:
- it requires a much lower dose for the same degree of antibody production
- it continues to induce the production of more antigen (spike protein) for a longer duration than existing mRNA vaccines like Comirnaty
I have long explained (for 25 plus years) that vaccines are unsuitable as a response to bioterrorism (or for that matter, rapidly mutating viruses) because you don’t know what the infectious agent will look like ahead of time, nor what the immunogenic epitopes on it will be—the area(s) against which a vaccine is directed. So you can’t design a vaccine ahead of time.
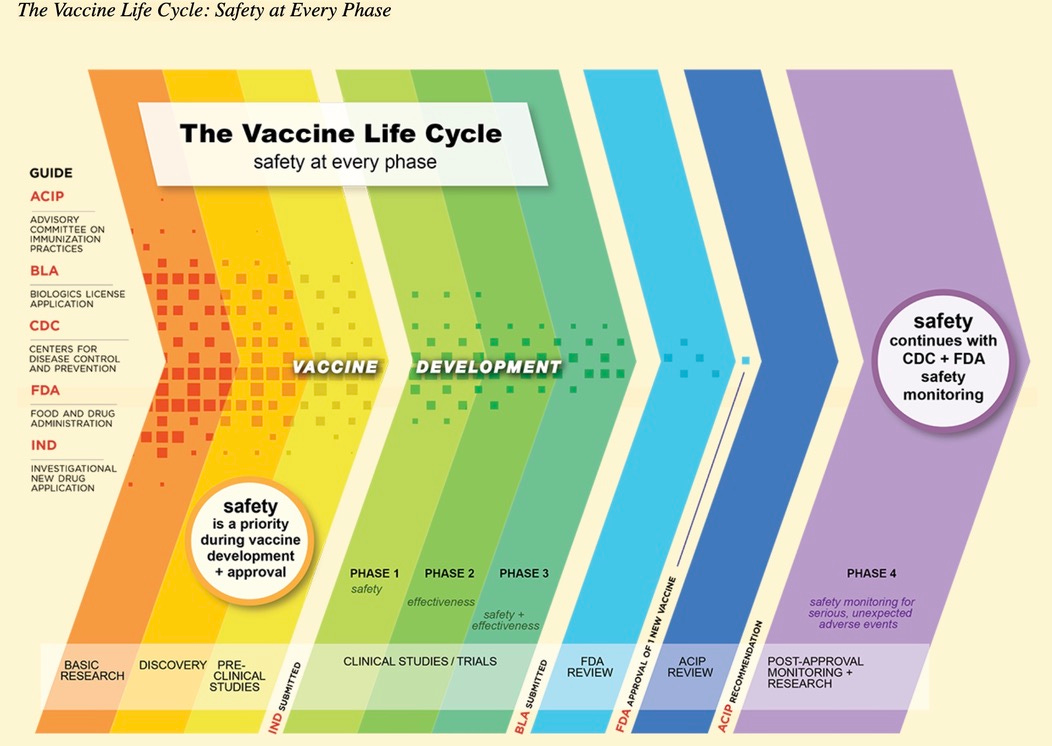
Furthermore, it takes years to assess the safety, efficacy and proper dose of a vaccine. So by the time you have been able to prepare and manufacture a vaccine the pandemic or biowarfare epidemic has come and gone.
Below is a [pre-COVID] CDC chart designed to show what happens during the 10-15 years it takes to develop a vaccine. Most vaccine candidates never make it to licensure because they are not safe or effective or require too high a dose to be economic.
Instead of admitting that producing a vaccine in time for an epidemic or biowarfare is impossible, grifters like Jeremy Farrar and Bill Gates, who together created the financial black hole CEPI (Coalition for Epidemic Preparedness Innovation) in 2017 to siphon $billions of our tax dollars for the 100 day vaccine moonshot, have simply behaved as if the limits of scientific innovation don’t apply to them.
They did not start with a new scientific advance. No, they started with a preposterous claim: We WILL produce a vaccine for pandemics or biowarfare in 100 days. And we will manufacture enough for the entire world in 30 more days.
How do you make this work? There is no new science. You make it work by killing regulation. Killing regulation works if you don’t actually care whether your product works or is safe. The original COVID vaccines seem to have been the test of whether you could make unsafe and ineffective vaccines and convince the public to take them.
Check.
But it took over 300 days to roll out the first Pfizer vaccines. So you need to use a platform that requires a smaller amount of product. The self-amplifying vaccine does that. That speeds up the manufacturing considerably.
If you can kill off a real regulatory process, you probably can manufacture enough of the self-amplifying vaccine for the whole world in 30 days. And you may make CEPI’s vaccine promise a reality.
You demand that every nation create a clinical trials network—the WHO and UN treaties attempted to include this but did not get the language to do so over the finish line. Ezekiel Emanuel has claimed it was a citizen duty to participate in clinical trials! And the 2016 21st Century Cures Act instructed FDA to use existing big data instead of clinical trials to speed up drug and vaccine licensure. In other words, the globalists have long viewed the traditional clinical trial process as a problem and tried to come up with ways to get around it.
What really happened for both the older COVID vaccines and the self-amplifying COVID vaccines (which Pfizer was studying in 2020 btw) is that very brief clinical trials were conducted, insufficient to generate evidence of safety or efficacy. Even then, Pfizer massaged its data, losing a huge number of vaccinated subjects but very few placebo subjects and mischaracterizing deaths and adverse events. Comirnaty’s clinical trial allegedly enrolled 40,000 subjects, but the data used by FDA to issue an authorization came from a mean enrollment of only two months.
The duration of enrollment for the Vietnam study of the self-amplifying mRNA vaccine was “up to three months” and averaged one month of followup after the first dose:
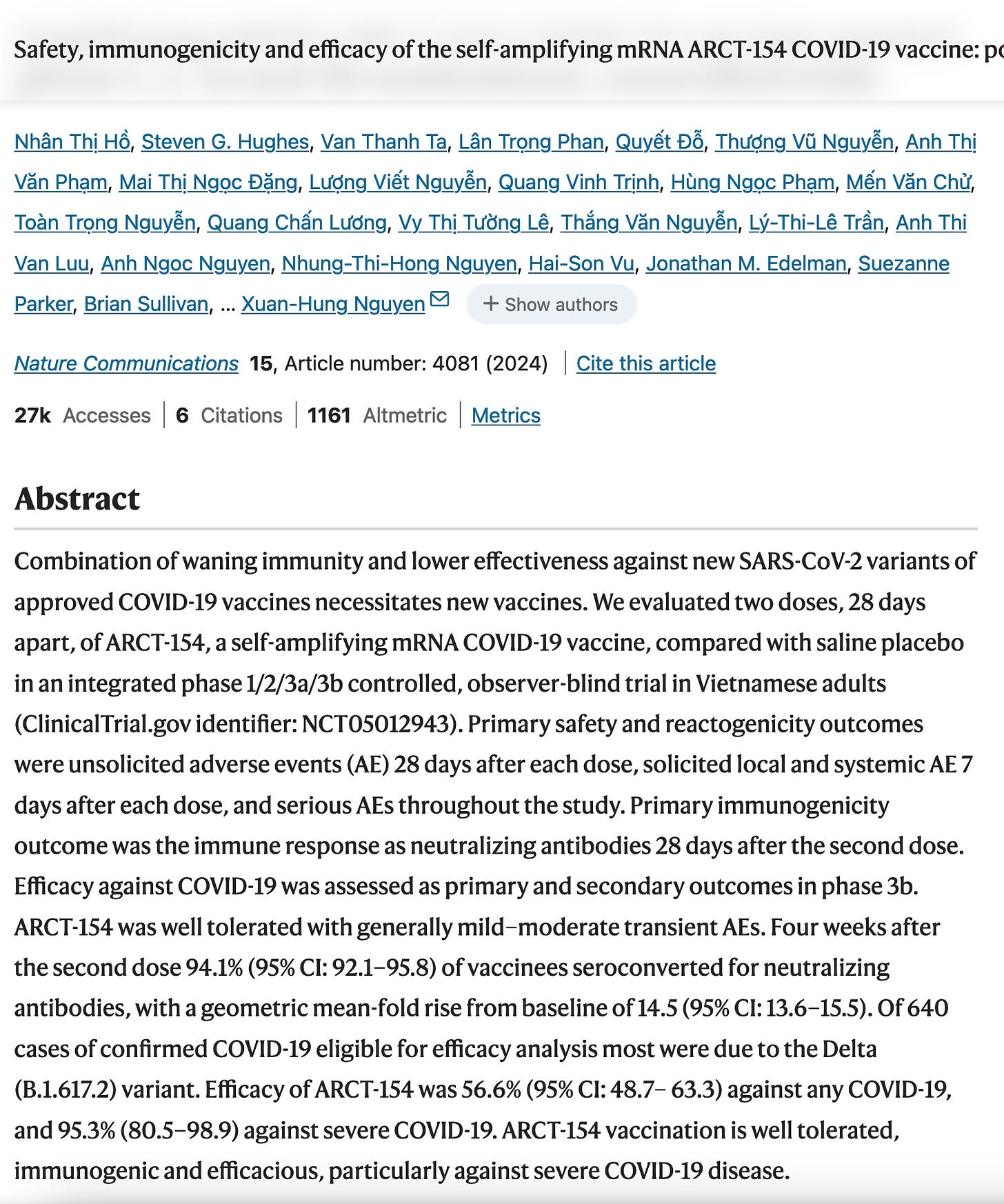
The placebo groups in 2 studies described in the paper above (one a pooled study of 1,000 subjects and the other a study of 16,000 subjects) allegedly had many more serious adverse events than the vaccinated subjects: 3.3 times as many in the first group, and 1.6 times as many in the second group. This reveals some significant problem with the study: perhaps the placebo injection caused problems, perhaps the placebo groups were sicker than the vaccinated groups, perhaps the investigators favored the vaccine groups and did not list all their adverse events… Whatever it was, this told me the study was unreliable and should not be considered in a licensing decision. The claim was made that the vaccine was 56% effective.
What about Arcturus? On its Board is the famous or infamous Dr. Moncef Slaoui, who was the Chief Scientific Advisor to Operation Warp Speed. He has been involved with a number of questionable vaccines it seems:
Under his leadership the operation enabled the fastest ever development, manufacturing, and approval of multiple COVID-19 vaccines in less than 11 months after the virus genetic sequence was described. Dr. Slaoui has sat on several biotechnology company boards, including Moderna, Inc. and Lonza Group AG, and he chaired the boards of Galvani, and Vaxcyte, a vaccine development platform company. Dr. Slaoui spent nearly 30 years at GlaxoSmithKline (GSK) holding leadership positions including as member of the Board of Directors of GSK PLC; Chairman of Pharmaceutical R&D; Chairman Global R&D, Vaccines & Oncology; and Chairman, Global Vaccines. As Chairman of Pharmaceutical R&D, Dr. Slaoui led a restructuring to improve focus on innovation and productivity. As Chairman of Global Vaccines, Dr. Slaoui was directly involved in GSK's vaccine pipeline, leading to the creation of 14 new vaccines, including Shingrix®, to prevent shingles; Cervarix®, to prevent cervical cancer; Mosquirix, to prevent malaria; Rotarix®, to prevent rotavirus gastroenteritis; and Synflorix, to prevent pneumococcal disease.
Arcturus just produced some longer-term, additional data about its vaccine:
What is the bottom line?
- The spike protein should not be used as an antigen for any vaccine due to its toxicity—but it is being used again, regardless.
- The LNP in this case has been around a long time and probably has roughly similar toxicity as the Pfizer and Moderna LNPs.
- Current mRNA COVID vaccines have net no efficacy (since their initial efficacy becomes negative after several weeks or months) and so a prolonged duration of spike protein production could mean even worse (more negative) efficacy—which should be settled before giving the vaccine to people.
In Japan, there is concern that the vaccine could spread or shed between people. Certainly, since this self-amplifying vaccine makes its own mRNA, this is a greater concern than with ordinary mRNA vaccines. Greater amounts of mRNA might be found in body fluids (including exosomes) or breath or excreted with urine and stool. Will the replicase enzyme (the rna dependent RNA polymerase) also be produced in large quantities? I do not know.
Japan is a country where there is a lot of knowledge about the risks of the mRNA vaccines. It appears that the new sa-mRNA vaccines, which rolled out at the start of October in Japan, are getting push-back from the people.

A new COVID-19 vaccine has sparked extreme anxiety among parts of the public, leading some businesses to deny services to those who have received the shot and causing at least one clinic to stop giving the vaccine for fear of being harassed.
The health ministry and experts say such fears — fueled by comments circulated both online and offline that the vaccine multiplies in the body indefinitely and as a result causes the “shedding” of its ingredients from an inoculated person to unvaccinated individuals — are unwarranted.
“There’s no scientific evidence that the replicon vaccine will make an infinite number of proteins in the body or its components will be transmitted to others,” the health ministry states on its website.
One of the five shots included in the government’s routine COVID-19 vaccination program, which began Oct. 1 and runs until the end of March, is the replicon vaccine Kostaive. Once inside the body, it uses a self-amplifying messenger RNA that creates proteins evoking immune responses against the coronavirus.
U.S.-based Arcturus Therapeutics developed Kostaive to address the shortcomings of earlier mRNA vaccines, which can only keep infection or the development of symptoms at bay for a few months.
The vaccine can evoke a stronger and more sustained immune response using a smaller dose than conventional mRNA vaccines, according to Meiji Seika Pharma, which manufactures and markets the shot in Japan.
In the last stage of a clinical trial using the vaccine as the initial shot, which was conducted in Vietnam during a delta variant wave and involving 16,000 people, Kostaive was shown to prevent the development of severe illness in 95.3% of those who received it while preventing symptoms from emerging in 56.6% of recipients.
In a separate trial for a booster shot comparing Kostaive and Pfizer’s Cominarty shot involving 828 people in Japan, the former was shown to sustain higher levels of antibodies, with comparable levels of side effects that were either minor or mild, according to data provided to the health ministry.
Japan was the first country to approve this “next-generation” mRNA vaccine, while the European Medicines Agency is currently reviewing Arcturus’ request for the vaccine’s approval in the European Union.
In Japan, fears about the vaccine’s safety have spiraled. In August, the Japan Nursing Ethics Association, a group of nursing ethics researchers, released a statement questioning the vaccine’s safety. The statement referred to the danger of vaccine shedding from the inoculated to the unvaccinated, quoting a paper published in a U.S. journal largely known for its opposition to vaccines.
The panic over shedding escalated last week, when the major yoga chain Lava announced an entry ban for those who have received this replicon vaccine “until its safety is confirmed.” Lava runs over 500 yoga studios across Japan.
One clinic in Tokyo’s Kita Ward even suspended reservations for the vaccine after it was inundated with threats and harassment from those protesting against the replicon vaccine.
“It has become difficult to respond to reservation inquiries about the world's first replicon vaccine,” the clinic, run by Dr. Hiromichi Ito, wrote on its website. “While we believe that the theoretical and scientific data (on the vaccine’s safety) are acceptable, the public opposition has been so extreme. We have received threats and slander on social media and harassing phone calls even late at night.”
Yuji Yamada, assistant professor of geriatrics at the Icahn School of Medicine at Mount Sinai in New York, called the nursing ethics association’s statement “pretty horrible,” saying it was given a false sense of authority by quoting a paper that may look reputable to some but which is scientifically flawed.
“The statement cites a paper in which the authors imagine that shedding could occur with this vaccine and say that there is concern about shedding, but in reality, there is no paper that has proven shedding at all.”
The word “shedding” is often used to refer to the transmission of a virus to humans through saliva or droplets after the virus replicates in the body. Yamada says there is no possibility of Kostaive causing the virus to be transmitted.
“This vaccine only contains mRNA that produces spike proteins, so it is impossible to create a complete virus,” he said.
In addition, mRNA easily breaks down in cells, so even if the vaccine’s mRNA lasts longer than other mRNA shots, it won’t keep multiplying forever, he said. Meiji Seika Pharma says the amplification period is short, noting that animal studies have shown significantly fewer mRNA at the injection site eight days after inoculation.
But some doctors have, for now, stopped short of actively recommending the replicon vaccine, given the abundance of other mRNA vaccines that have been used around the world and whose safety has been well established.
Yamada added that, in general, the use of the self-amplifying vaccine is not advisable for people taking immunosuppressants and pregnant women, as clinical studies have so far excluded them.
“It’s just that the data (involving these groups of people) aren’t fully there yet for the vaccine, so I would recommend other options,” he said.
Setting aside safety concerns, Kostaive won’t probably be widely available this year anyway, Yamada said, noting that small clinics administering COVID-19 shots are shying away from stocking the vaccine for financial reasons.
As one vial of Kostaive contains 16 doses, some clinics are worried about the prospect of not using up all the doses within one month, the period during which an unsealed vial can be kept, he said. If they do not use up their doses, the clinics could lose money.
Until April, COVID-19 vaccinations were classified as temporary inoculations and offered for free, with the central government paying the full cost. Since this month, COVID-19 shots have been administered as part of an annual routine inoculation program similar to seasonal flu shots.
COVID-19 shots are recommended for people age 65 or older and those between the ages of 60 and 64 with severe underlying conditions. The health ministry subsidizes the shots to cap out-of-pocket expenses at ¥7,000 ($47), and some municipalities offer subsidies to bring the fee down or offer them for free.
International organizations sprout like mushrooms to echo each others' false narratives and pay the bills. MPOX, the GPMB, WHO, UN and World Bank, and their incestuous relationship
“The UN system is comprised of more than 30 affiliated organizations, programs, funds, and specialized agencies, with their own membership, leadership, and budget processes. These entities work with and through the UN Secretariat to promote peace and prosperity.
UN funds and programs are financed through voluntary rather than assessed contributions.”
This allows nations to donate to many different agencies without citizens being aware the money is all going to practically the same place and the same group of people to push a similar set of policies.
But these 30 UN-associated entities, which include the World Bank, are not enough to get the globalist program pushed through globally. After all, they do have rules about giving jobs to people from around the world, and letting member nations appoint staff, and so there can be push-back within the agencies against various globalist agendas.
So new institutions were formed, sometimes connected to these UN agencies, sometimes allegedly connected or unconnected, sometimes as donors or as think tanks, to steer policy internationally as well as within the UN system itself. Just as we have so many NGOs in Washington whose purpose is to steer US policy.
Many of these new institutions were created since 2000, by people like Bill Gates: GAVI, CEPI, etc. Some are older organizations that Bill Gates has basically co-opted and taken over, via donations, like CGIAR, supposed to help developing countries with agriculture, but now focused on climate change:
Some were created as partnerships by the Wellcome Trust, which also stepped up its game at the WHO in 2018:
Building on many years of collaboration, Wellcome became a non-state actor in official relations with the WHO in February 2018. This means we can play a more active part in WHO processes, for example by participating at sessions of its governing bodies and organising side events.
At a strategic meeting with the WHO in November 2018 we identified our shared goals, and the experience, networks and resources we can pool to work on them together.
Strategic priorities
Our partnership with the WHO focuses on:
- epidemics and other health emergencies
- antimicrobial resistance
- global health research and development.
Pretty obvious what WELLCOME (then under the stewardship of Jeremy Farrar) was doing to control the WHO agenda: grabbing the epidemic/pandemic space, pushing One Health with the antimicrobial resistance bogeyman that has failed to materialize as a significant threat but is kept alive through bad animal husbandry practices, and global health R and D, whatever they mean by that.
Then there are independent organizations that are tenuously related to the WHO and World Bank to provide the new organization with cachet, otherwise we would ask, “Who made you the boss of me?”
The Global Preparedness Monitoring Board (GPMB) is such an “independent” organization. The GPMB was established in 2018 following the recommendation of the High-Level Panel on the Global Response to Health Crises, a committee appointed by the UN Secretary-General in 2015 and tasked with calling for a GPMB.
The Global Preparedness Monitoring Board (GPMB) is an independent monitoring and accountability body to ensure preparedness for global health crises. Co-convened by the Director-General of the World Health Organization and the President of the World Bank, the GPMB is comprised of globally-recognized leaders and experts from a wide range of sectors, including global health, veterinary epidemiology, environment, human rights, economics, law, gender, and development.
It is tasked with providing an independent and comprehensive appraisal for policy makers and the world about progress towards increased preparedness and response capacity for disease outbreaks and other emergencies with health consequences. In short, the work of the GPMB is to chart a roadmap for a safer world.
https://www.gpmb.org/about-us#tab=tab_1
The Board is also responsible for producing a Monitoring Framework that provides a single, authoritative, and actionable roadmap for global preparedness.
Get it? We will be your single voice for truth about pandemic preparedness. We own the science. We will monitor your compliance. The GPMB is also an entity working behind the scenes to get the WHO Pandemic Treaty etc. pushed forward.
It is mind-boggling how many of these spin-off organizations there are. Here is another one, created in 2021: G20 High Level Independent Panel on Financing the Global Commons for Pandemic Preparedness and Response.
But back to the GPMB. Who were its leaders when it was founded 6 years ago? Here are just 5 of about a dozen:
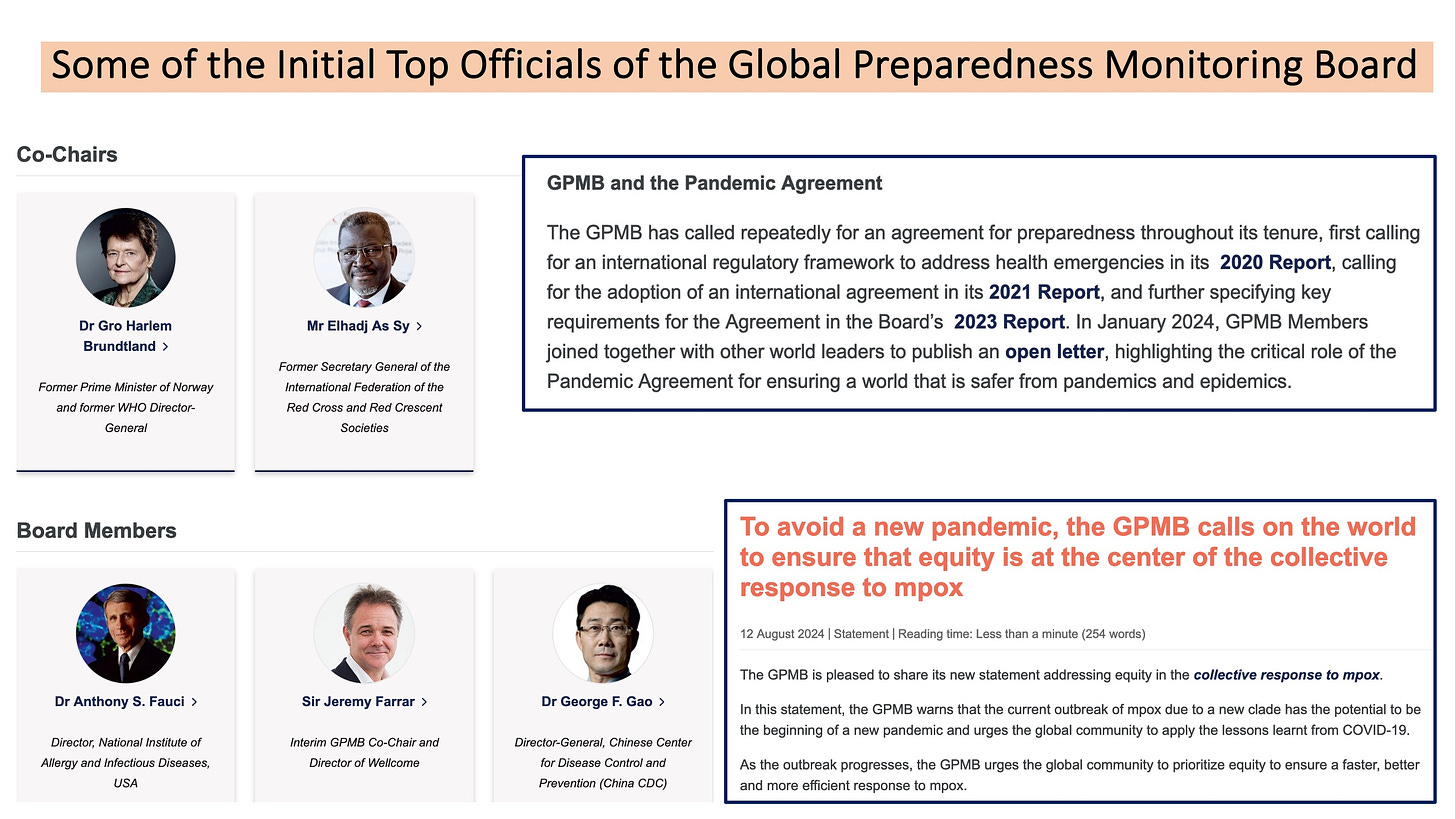
I talked about Gro in Japan and James Corbett also featured her, the creator of Sustainable Development (which has nothing to do with development) and climate globalist extraordinaire.
Mr. As Sy is not a medical person, but he is a loyal apparatchik who was included in many of Fauci’s (FOIA’ed) emails early in the pandemic.
The rest are all MDs. George Gao, who was then head of the Chinese CDC, is an old buddy of Jeremy Farrar’s from Oxford. He attended the Event 201 exercise in 2019 and the monkeypox tabletop exercise in early 2021. You know Jeremy and Tony Fauci already.
This little group was intended to set the entire world on the right course regarding pandemics and biowarfare and the WHO.
Those members moved on, though there remain some power players on the GPMB now. They are trying hard to stay relevant. Today they issued a report, which the WHO released. In August 2024 they tried to build up Monkeypox as a big threat requiring “equity,” i.e., vaccines for Africa, free and lots of them:
However, today the WHO had to admit, yet again, that they can’t find confirmed deaths from $moneypox. Zero deaths over the past 6 weeks with confirmed monkeypox, though there are hundreds of deaths they are guessing might have had monkeypox.
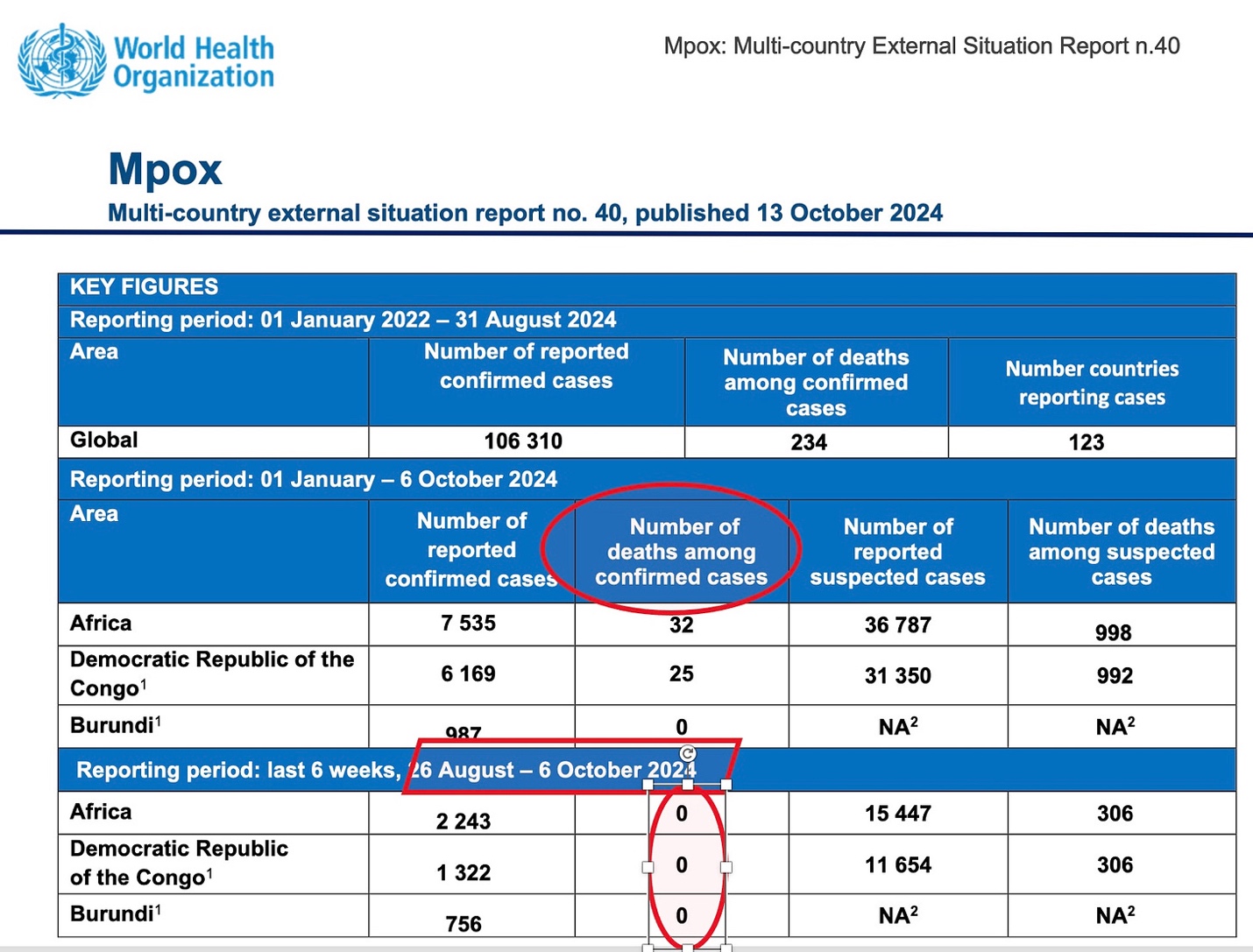
(I love being proven right.) Below is today’s report from the GPMB, just so you know they continue to try and remain relevant and authoritative.
The other thing they are desperately trying to do is to counter the REPPARE reports by David Bell et al. that showed pandemics are essentially irrelevant to public health, as so few people overall have been affected over recent decades, if you don’t include lab-derived COVID. Here is REPPARE’s latest report, but there are more here, which completely dispute the GPMB, WHO and the other false, hyped narratives about the dangers of pandemics.
Here is the GPMB’s press release of today, bolded by me:

Monday, 14 October 2024
As co-convenor with the World Bank Group, WHO is sharing this press release and report, on behalf of the Global Preparedness Monitoring Board (GPMB). Interviews with the Board members are available on Monday, 14 October. Please contact Kate Thompson (thompsonk@who.int) or John Butler (butlerj@who.int) for more details.
PRESS RELEASE
New risks raise pandemic threat on a global scale
14 October 2024 – Recent outbreaks of Marburg virus, Mpox and the latest strain of avian influenza (H5N1) are a stark reminder of the world’s vulnerability to pandemics. In 2024 alone, 17 outbreaks of dangerous diseases have already occurred. Each new outbreak exposes fault lines in the existing pandemic prevention architecture and global readiness to respond to disease outbreaks.
A plethora of risks increase the likelihood of new pandemics according to a new report from the Global Preparedness Monitoring Board (GPMB). The report, launched at the 15th World Health Summit in Berlin, outlines 15 key drivers of pandemic risk, categorized into five distinct groups: social, technological, environmental, economic, and political.
GPMB, an initiative supported by the World Health Organization and the World Bank, tracks the drivers of pandemic risk and oversees global preparedness. The report stresses the urgency of understanding the global vulnerability to threats and calls for a radical reset of the collective approach to pandemic preparedness.
Lack of trust between and within countries, inequity, intensive farming and the likelihood of human to animal crossover are among the key threats outlined in the report. The report also identifies new risks outside of the traditional health factors.
Digital connectivity has enabled scientists to quickly sequence and share pathogen data and tailor responses ever faster. However, this digital footprint leaves health systems and societies exposed. Cyber-attacks, heightened biosecurity threats, and the rapid spread of misinformation all increase the risk of a pandemic.
“The next pandemic won't wait for us to perfect our systems,” said Joy Phumaphi, GPMB Co-Chair and former Minister of Health to Botswana. “We must invest now in resilient and equitable primary healthcare systems to withstand the challenges of tomorrow.”
The report identifies the complex and interdependent factors which shape the risk of pandemics. However, it also stresses that willingness to build flexibility into the response, proactively protect society and invest in collaborative efforts can significantly reduce risk and enhance preparedness.
To effectively protect themselves, all nations must strengthen their health systems, prioritize social protection, and ensure that essential health services are available to all communities, particularly the most vulnerable and disadvantaged. GDP alone is no measure of resilience to a pandemic.
Preparedness should incorporate strategies spanning across the human, animal, and environmental health interfaces. The report calls for increased collaboration across sectors to mitigate risks associated with pandemics, recognizing that the health of one sector is intricately linked to the health of others. [The One Health fairy tale—Nass]
“We have a narrow window of opportunity to rethink global preparedness: to assess risks that extend well beyond the health sector, and to address some of these far more proactively, in a way that is adapted to each context,” said H.E., Ms. Kolinda Grabar-Kitarović, GPMB Co-Chair and former President of Croatia. “Vigilance, adaptability and collaboration must define our preparation now, so that is it baked-in to the response”.
The report provides a framework for policymakers to adapt existing health strategies and enhance protective measures against future pandemics. This includes ensuring prevention and response plans are regularly reviewed and flexible enough to respond to all situations. The next pandemic will not follow the same path as COVID-19, lessons learned from that experience should guide but not define preparedness.
Resilience in future health emergencies is contingent on investment in research and development, improved technology, equitable health infrastructure and an enhanced understanding of the dynamic nature of all pandemic risk drivers. In today’s interconnected world, the global community must take collective responsibility for prevention and response to disease, rather than considering preparedness as an individual country or sector-level activity.
The report is available on the GPMB website.
Note to editors:
The Global Preparedness Monitoring Board (GPMB) is an independent monitoring and accountability body to ensure preparedness for global health crises. Co-convened by the Director-General of the World Health Organization and the President of the World Bank, the GPMB is comprised of globally recognized leaders and experts from a wide range of sectors, including health, animal health, environment, human rights, economics, law, gender, and development. It is tasked with providing an independent and comprehensive appraisal for policy makers and the world about progress towards increased preparedness and response capacity for disease outbreaks, epidemics, and pandemics. In short, the work of the GPMB is to chart a roadmap for a safer world.