
First, it should be noted that the names used for this document change with each draft, which is very confusing. The current draft is titled:
Advanced unedited version – 16 October 2023
This document is very similar to the June 2 “Bureau Draft” and so I enclose a copy of my analysis of that document also, as it provides additional detail. But it should be understood that this treaty is based on fantasy, as none of its foundational assumptions is accurate. The Pandemic Treaty intends to create a complicated managerial structure with a new WHO Secretariat and Conference of the Parties to perform activities that have never been shown to prevent or respond to pandemics effectively or provide any other benefits. In fact, these efforts are most likely to increase pandemics and encourage the use of hasty regulatory structures and problematic, liability-waived vaccines produced too quickly.
All the Pandemic Treaty drafts so far rely on a set of incorrect assumptions. They include the following:
- The WHO is the directing and coordinating authority on international health.
- International spread of disease demands the widest international cooperation, ignoring the fact that international spread may be limited to only a few countries and will demand a different level of response, depending on the circumstances.
- Nations retain national sovereignty through their ability to pass health laws, while they will simultaneously be bound and accountable to obey the directives from the WHO on health.
- We were unprepared for COVID and this caused the pandemic’s suffering, but now we know how to prepare for pandemics and simply need a central authority to direct us.
- Lack of equity led to failure to share drugs, vaccines, PPE — ignoring the fact that no nation had sufficient PPE or tests early in the pandemic, and that it was nations withholding generic drugs from their populations, not lack of equity, causing many treatment shortages.
- Pandemics invariably arise at the animal-human interface, are natural in origin, and the vaguely defined “One Health approach” can prevent or detect them early.
- Increasing the capture and study of “potential pandemic pathogens” can be done safely and provide useful pandemic products, when neither has been true in the past.
- Pharmaceutical manufacturers will agree to give up some intellectual property rights. In fact, a Pharma manufacturers’ association said this week it would prefer no treaty to this one.[1]
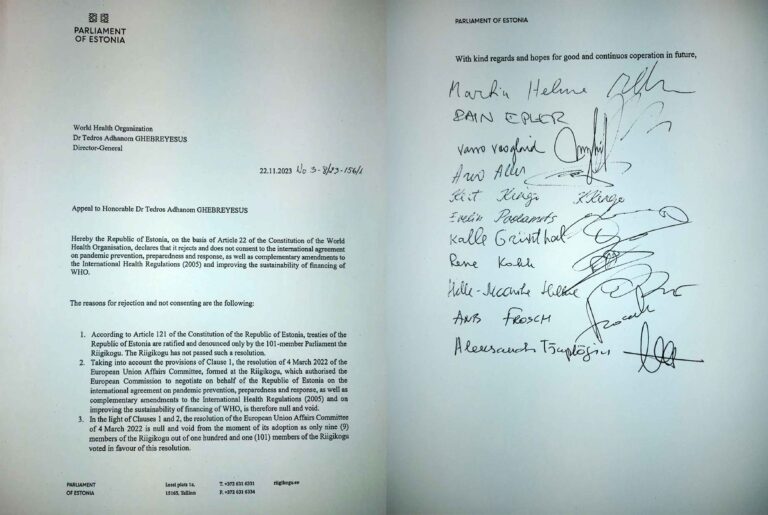
- The UN adopted a declaration on pandemic preparedness on September 20, 2023. In fact, 11 countries objected and the declaration was only approved by the UN Secretary-General.
- Censorship of “infodemics” is legal and desirable.
- Nations and the WHO must apply the “One Health approach,” which includes efforts related to climate change and sustainable development, for health promotion.
- Health “coverage” (insurance) will provide the world’s citizens access to a broad range of health care.
Here are some specific examples of what is wrong with the Treaty.
Article 3, #2. Sovereignty
“States have, in accordance with the charter of the United Nations and the general principles of international law, the sovereign right to legislate and to implement legislation in pursuance of their health policies.” This language fails to address the issue of the WHO assuming sovereignty for health matters over states through this treaty.
Article 3, #3. Equity
“Equity includes the unhindered, fair, equitable and timely access to safe, effective, quality and affordable pandemic-related products and services, information, pandemic-related technologies and social protection.” However, Article 9, #2 (d) states that parties shall promote “infodemic management,” and infodemic is defined in Article 1(c) as false or misleading information. Article 18, #1 instructs the Parties to “combat false, misleading, misinformation or disinformation…” In earlier drafts the WHO spelled out that only the WHO’s public health narrative would be allowed to spread.
Article 4, #3. Pandemic prevention and public health surveillance
“The Parties shall cooperate with the support of the WHO Secretariat to strengthen and maintain public health laboratory and diagnostic capacities, especially with respect to the capacity to perform genetic sequencing, data science to assess the risk of detected pathogens and to safely handle samples containing pathogens and the use of related digital tools.” While this language is more spare than in previous drafts, it does direct nations to perform genetic sequencing of potential pandemic pathogens (i.e., biological warfare agents) they find and to safely handle them, which requires high containment (BSL3/4) laboratories.
Also in Article 4 is the need to “develop, strengthen and maintain the capacity to (i) detect, identify and characterize pathogens presenting significant risks…” indicating the directive for nations to perform surveillance to seek out such pathogens.
Article 6, #4. Preparedness, Readiness and Resilience
“The Parties shall establish, building on existing arrangements as appropriate, genomics, risk assessment, and laboratory networks in order to conduct surveillance and sharing of emerging pathogens with pandemic potential, with such sharing pursuant to the terms and modalities established in Article 12.” Article 1 (h) defined “pathogen with pandemic potential” as any pathogen that has been identified to infect humans and that is potentially highly transmissible and capable of wide, uncontrollable spread in human populations and highly virulent, making it likely to cause significant morbidity and or mortality in humans.” Why does the WHO require nations to go out and find potential pandemic pathogens (a.k.a. biological warfare agents) and supply both samples and their sequences to the WHO, where they will be shared with pharmaceutical companies, research centers and academic institutions, as well as possible others and online?
Article 8, #3. Preparedness monitoring and functional reviews
“The parties shall, building on existing tools, develop and implement an inclusive, transparent, effective and efficient pandemic prevention, preparedness and response monitoring and evaluation system.” Yet four different monitoring systems have been used to gauge nations’ readiness for pandemics and all four failed to predict how well they would do when COVID appeared. There is no acknowledgement of the failures of our assessment tools, nor discussion of whether there exist any useful assessment tools.[2] [3] And this begs the question why, if our means of assessing progress against pandemics failed, do we think that similar efforts are likely to be successful in future?
Article 10, #1 (d). Sustainable production
“The Parties encourage entities, including manufacturers within their respective jurisdictions, in particular those that receive significant public financing, to grant, subject to any existing licensing restrictions, on mutually agreed terms, non-exclusive royalty-free licenses to any manufacturers, particularly from developing countries, to use their intellectual property and other protected substances, products, technology, know-how, information and knowledge used in the process of pandemic-related product development and production, in particular for pre-pandemic and pandemic diagnostics, vaccines and therapeutics for use in agreed developing countries.” This and related sections are probably what make the pharma organization so upset with the Treaty.
Article 12, #4 (a) i (2) Access and benefit-sharing
“Each Party, through its relevant public health authorities and authorized laboratories, shall, in a rapid, systematic and timely manner: …(2) upload the genetic sequence of such WHO PABS (Pathogen Access and Benefits System) material to one or more publicly accessible databases of its choice, provided that the database has put in place an appropriate arrangement with respect to WHO PABS material.”
There is additional discussion about the sharing of pathogens and the need to identify and upload their genetic sequences online where they will be accessible. This could also be called proliferation of biological weapons agents, which is generally considered a crime. In the US, “Select Agents” are those designated to have pandemic potential, and the select agent program [4] is managed by CDC and USDA. For safety, CDC must give permission to transfer select agents. Yet the select agent rules are ignored in this WHO Treaty.
And in an apparent effort to handwave over existing rules, the drafts says in Article 12, #8, “The Parties shall ensure that such a system is consistent with, supportive of, and does not run counter to, the objectives of the Convention on Biological Diversity and the Nagoya Protocol thereto. The WHO PABS system will provide certainty and legal clarity to the providers and users of WHO PABS materials.”
Article 13, #3 (e). Global Supply Chain and Logistics
“The terms of the WHO SCL Network shall include: facilitating the negotiation and agreement of advance purchase commitments and procurement contracts for pandemic-related products.” Advance purchase commitments are contracts that obligate nations to buy products for pandemics in advance, sight unseen. Neither the manufacturer nor the nation knows what is coming, but once WHO issues a pandemic declaration, the contracts are activated and the US government will have to buy what the manufacturer produces. The 2009 swine flu pandemic provides a useful example. Advance purchase commitments led to tens of $ billions in vaccine purchases in North America and Europe for a flu that was less severe than normal. The GSK Pandemrix brand of vaccine led to over 1300 cases of severe narcolepsy, primarily in adolescents. [5] Rapid production of vaccines for which profits are guaranteed and liability is waived has never been a win for the consumer.
Article 14. Regulatory Strengthening
Nations are to harmonize their regulatory requirements, expedite approvals and authorizations and ensure the legal framework is in place to support emergency approvals. This incentivizes a race to the bottom of drug and vaccine approval standards, particularly during emergencies.
[1] https://www.ifpma.org/news/innovative-pharmaceutical-industry-statement-on-draft-who-pandemic-treaty-we-need-to-preserve-what-went-well-and-address-what-went-wrong/ “As the body representing the global innovative pharmaceutical industry in official relations with the United Nations, IFPMA has issued the following statement in response. IFPMA Director General, Thomas Cueni said on October 17, 2023:
“It would be better to have no pandemic treaty than a bad pandemic treaty, which the draft circulated to member states clearly represents.”‘
[2] WHO Report: Independent Oversight and Advisory Committee for the WHO Health Emergencies Programme.
Interim report on WHO’s response to COVID-19 January-April 2020.
“The IOAC sees no clear relation between JEE scores and country preparedness and response to COVID-19, suggesting that existing metrics for public health preparedness and health care capacity do not reflect the full range of variables that affect a country’s response during a severe pandemic on a massive scale. The majority of countries appeared ill-prepared and struggled to implement public health measures in response to COVID-19. In the light of this pandemic, the IOAC recommends that Member States and the WHO Secretariat 6 review the IHR core capacities and existing tools and framework for national and international preparedness, and consider whether they need to be updated.”
[3] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9111134/
[4] https://www.selectagents.gov/
[5] https://www.science.org/content/article/why-pandemic-flu-shot-caused-narcolepsy