This article is a repost with permission from The Defender
The U.K. is weighing an initiative to rubber stamp drugs already sanctioned abroad, but critics warn the plan undercuts safety standards and signals a move toward the World Health Organization’s “One Health” strategy.
The U.K.’s drug regulator, the Medicines and Healthcare Products Regulatory Agency (MHRA), is weighing a plan that would result in what The BMJ has described as “near automatic sign off” for medicines “already approved by ‘trusted’ regulators in other parts of the world.”
The proposal is raising concerns among some medical experts.
According to a JD Supra article, these “new international recognitions routes” announced by the MHRA are intended for the quick “approval of medicines that are already authorised in Australia, Canada, the European Union (EU), Japan, Singapore, Switzerland or the United States.” The new “routes” are expected to begin by Jan. 1, 2024.
Medications already licensed in any of these “trusted partner” countries would receive “a fast-track U.K. application process.”
The plan builds on the MHRA’s existing European Commission (EC) Decision Reliance Procedure and also “complements the U.K. national authorisation process and accelerated access route, the Innovative Licensing and Access Pathway (ILAP).”
This procedure was introduced following Brexit to allow the MHRA to “rely” on drug approvals from the European Medicines Agency (EMA). If a drug has received EMA approval or a “positive recommendation,” the MHRA can then proceed with a “lighter touch” assessment and “accelerated decision from the MHRA within 67 days or less.”
In March, the U.K. government awarded the MHRA £10 million ($12 million) in funding “to help bring innovative new medicines and medical technologies to U.K. patients more quickly.”
Describing this new process as a “milestone,” JD Supra claimed it “is intended to result in faster access for U.K. patients to new innovative medicines.”
The Association of the British Pharmaceutical Industry said the process will reduce “the time delay for regulatory approval.”
Regulators want to ‘please Big Pharma’
Medical and vaccines experts who spoke with The Defender, however, expressed concerns over safety risks associated with an expedited approvals process and a reduction in regulatory oversight.
Dr. Meryl Nass, an internist, biological warfare epidemiologist and member of the Children’s Health Defense (CHD) scientific advisory committee, told The Defender, “The process of ‘harmonizing’ laws and standards between countries — beyond just the EU countries — has been ongoing for years.”
However, “By saying that any friendly nation’s drug regulator decision can stand in your country — well, that obviously will turn into a race to the bottom,” she said, implying that there would be continuous increased pressure to hasten drug development and approvals.
Barbara Loe Fisher, co-founder and president of the National Vaccine Information Center and co-author of the 1985 book “DPT: A Shot in the Dark,” told The Defender:
Over the four decades that I have been an informed consent advocate in the U.S., I have watched Congress direct federal agencies to develop public-private business partnerships with pharmaceutical companies.
This has led to a systematic lowering of the bar requiring companies to demonstrate new vaccines are safe and effective before licensure so they can be rushed to market, recommended for universal use, and often mandated.
Fisher gave the example of previously “fast-tracked” vaccines that resulted in bad outcomes for public health. She said:
Licensed in 2006, Merck’s Gardasil was the first “fast-tracked” vaccine to be licensed by the FDA [U.S. Food and Drug Administration] using an accelerated approval process.
But the mRNA COVID biological was the first to be approved for public use under an Emergency Use Authorization (EUA) after only nine months of study and it has already racked up a record 1.5 million adverse event reports to the Vaccine Adverse Event Reporting System (VAERS) while making billions of dollars in profit for companies.
VAERS has historically been shown to report only 1% of actual vaccine adverse events.
Nass referred to a June 2022 BMJ article, “From FDA to MHRA: are drug regulators for hire?” that found “industry money permeates the globe’s leading regulators, raising questions about their independence, especially in the wake of a string of drug and device scandals.”
For instance, the FDA, despite being the most highly funded of the six regulatory authorities studied, receives 65% of its funding for drug evaluation from industry “user fees.”
In 1995, the EMA received just 20% of its funding from industry fees. That figure has since grown to 89%.
Australia’s industry-funded portion of their regulatory budget — 96% — exceeds all other countries. During 2020-2021, Australian regulators approved more than 90% of drug applications.
Canada’s regulatory authority receives the smallest percentage of industry funding among the six “international recognitions route” countries, yet even that amount exceeds half (50.5%) of its budget.
“Unfortunately, Big Pharma has been allowed to capture and corrupt the government regulatory process in the U.S. and in other countries doing business with that industry,” Fisher said. “The quick rubber stamping of new vaccines being rushed to market will continue to put the public health and safety at risk until lawmakers act to end it.”
“The regulators are already beholden to private industry,” Nass said. “They don’t do a credible job anymore, and so they are taking the next step and ending regulation once and for all,” Nass said.
She cited the example of Peter Marks, M.D., Ph.D., head of the FDA’s Center for Biologics Evaluation and Research, who recently overruled the agency’s reviewers in granting accelerated approval to a gene therapy treatment for young children.
According to Nass, Marks “overruled his experts to please Big Pharma and license a drug that it shouldn’t.”
‘Vaccines in 130 days, anyone?’
Experts also connected fast-track drug approval to the Biden administration’s new national biodefense strategy, which calls for the development of vaccines within 130 days during pandemics and health emergencies.
Announced in October 2022, the “National Biodefense Strategy and Implementation Plan for Countering Biological Threats, Enhancing Pandemic Preparedness, and Achieving Global Health Security” is an $88 billion program calling for the rapid development and deployment of new vaccines and diagnostics in response to future “biological threats.”
The plan’s targets include developing the ability to test for new pathogens within 12 hours, making rapid tests available and repurposing existing drugs within 90 days, developing vaccines within 100 days and new treatments within 180 days, and manufacturing enough of the new vaccine to inoculate the entire U.S. population within 130 days.
Other goals contained within the plan include “detecting the spread of pathogens before patients even begin to show symptoms like fever” and “scaling up the number of diagnostic test kits by tens of thousands within a week.”
“Vaccines in 130 days, anyone?” Nass asked in a blog post connecting the Biden administration’s biodefense strategy to the MHRA’s plan for the “near-automatic” approval of drugs and treatments already approved by “trusted” nations’ regulators.
Along the same vein, Brian Hooker, Ph.D., P.E., senior director of science and research for CHD, told The Defender:
The whole prospect of rolling out a vaccine in 130 days is completely unrealistic and too many corners will be cut in order to accomplish this. Obviously, long-term safety studies will be non-existent.
Unfortunately, this will predictably lead to widespread vaccine injury and death as more and more untested products will be foisted on the public.
Nass told The Defender that such procedures will “probably” lead to new vaccine mandates for the general population. She added that, within a 130-day timeline, “no human testing at all” can be performed, “which means no safety testing, because safety testing cannot be done in animals. It’s not possible, as the regulators well know.”
‘Near-automatic’ drug approvals tied to WHO global initiatives
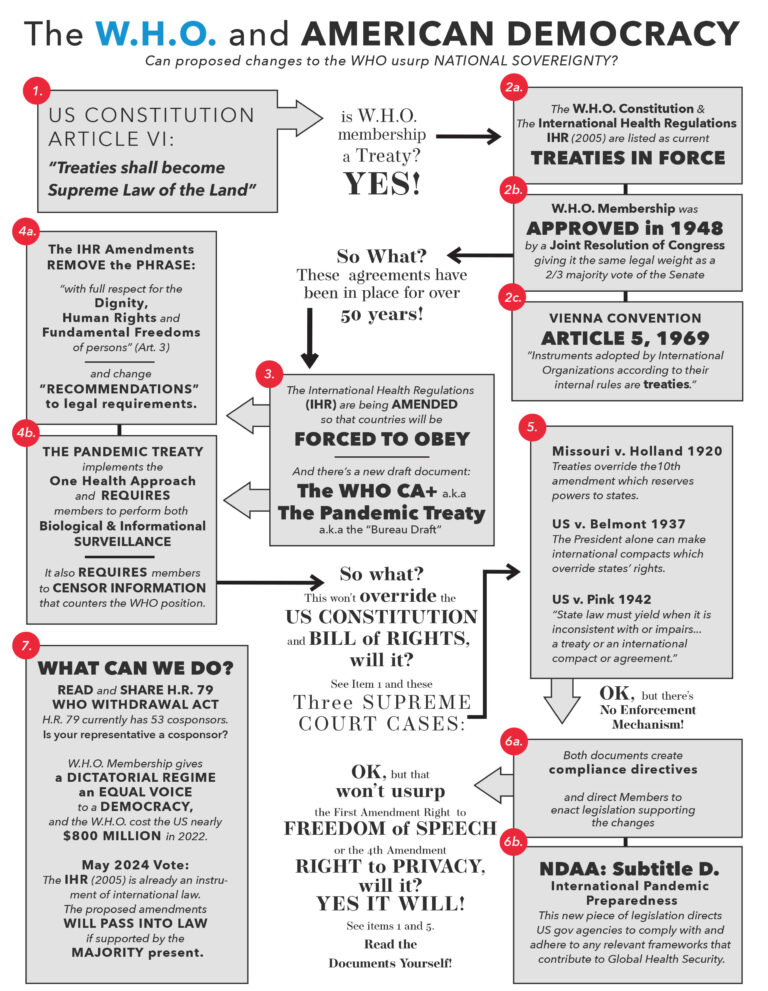
Medical experts also connected the MHRA’s plan to the controversial proposed amendments to the World Health Organization’s (WHO) International Health Regulations (IHR).
Current proposals for the IHR amendments include language implying that WHO member states will be obliged to coordinate their approval processes for drugs and treatments, particularly during a pandemic or health emergency.
For instance, the proposed Article 13A, Section 5 states:
“Upon request of a State Party, other States Parties or WHO shall rapidly cooperate and share relevant regulatory dossiers submitted by manufacturers concerning safety and efficacy, and manufacturing and quality control processes, within 30 days.
“The dossiers received by a requesting State Party shall be solely used by their regulatory authorities and manufacturers designated by the requesting State Party for the purposes of accelerating the manufacture and supply of product(s) or technology(ies) as well as expediting their regulatory approval.”
WHO member states are expected to vote on a final set of proposed IHR amendments during the World Health Assembly in May 2024.
Similarly, the White House’s newly announced Office of Pandemic Preparedness and Response Policy will be tasked, in part, with “development of next-generation vaccines.”
On her blog, Nass wrote MHRA plan is “One World governance … being ushered in through the back door.” She told The Defender, “The WHO IHR plan is a liability waiver” in and of itself.
Similar initiatives are also taking shape globally. The United Nations Pandemic Prevention, Preparedness and Response proposal is scheduled to be discussed by the U.N. General Assembly in September 2023.
The WHO proposal states:
“Member States … have agreed to a global process to draft and negotiate a convention, agreement or other international instrument under the Constitution of the World Health Organization to strengthen pandemic prevention, preparedness and response.”
For Nass, the MHRA’s new plan and global “pandemic preparedness” initiatives are being pursued because it is “the easiest way to give us more untested vaccines and drugs, liability-free, while having governments pay the costs so they can be mandated — since the government cannot order you to buy something.”