
Dear Friends,
The World Health organization held its annual meeting of member states the final week of May. In addition to its usual business, the WHO attempted to finalize major amendments to its existing International Health Regulations and pass a new Pandemic Treaty. Some people said this was the most important business the WHO conducted since its formation in 1948.
Under the guise of “equity,” it was claimed that these two documents would guarantee poor nations the products they might need during a future global pandemic. But under pressure from pharmaceutical companies, whose share prices had fallen after COVID, and unwillingness from the richer nations to foot the bill, no drafts of either document actually included such guarantees. Poorer nations were only offered 10% of pharma production for free, and 10% at a low price. They were expected to pay full price for the rest. As part of this deal, all nations were to agree to a variety of conditions designated as necessary for “pandemic preparedness,” many to be identified by committees that did not yet exist. The cost of compliance was unknown, while vague promises to help poorer countries meet these demands never got into the specifics in any drafts.
Attempts to water down both documents were made during the final days before and even during the meeting, but no general agreement could be obtained. Finally, at the eleventh hour (as often happens) an agreement was reached to give the Pandemic Treaty negotiations another year, with some new negotiators to be brought in. A set of amendments to the International Health Regulations were passed, but the heart of the document had been defanged: while the WHO Director-General would be allowed to declare public health emergencies, he would not accrue special powers as a result; he would not be able to order nations to pass laws; he could not issue lockdowns, mandates, etc. The details are below.
The globalists who were using the WHO as their pawn were far from happy with the proceedings. So unhappy, in fact, that they pulled out two UN/WHO hench-women (leaders of the so-called "Independent Panel” that is not at all independent, as revealed by its funding by Gates and Soros) to put their names on a new report, just issued, that begs the world to accept the WHO’s pandemic preparedness agenda. They have echoed the usual malarky that the world is not prepared for the next pandemic, and if we just spend enough money, and agree with their chosen path forward, we will become safer. However, granting the WHO the privilege to host a network of laboratories studying and sharing “potential pandemic pathogens” will make us anything but safe.
The Independent Panel’s report claims:
"This latest report evaluates the status of pandemic preparedness and response reforms and charts a path forward towards protecting all people around the world from future pandemic threats.”
and
“There must be action now —to close the gaps that put 8 billion people at risk of a new pandemic. The recent jump of the avian H5N1 virus to more mammals—including new human cases transmitted from cattle in the United States—portends an influenza pandemic the world is nowhere near ready to manage."
Door to Freedom is busy working on our own reporting of the avian H5N1 (Bird Flu) issue, and how it has been used for twenty years to generate pandemic fears, cull hundreds of millions of chickens, turkeys and ducks, and to justify the production of “pre-pandemic” vaccines to feed the biodefense industry, unsupported by science. The NIH has sponsored scientists around the world to create human-transmissible versions of bird flu. You will hear much more about this from us in the coming days and weeks.
The unhappy globalists also got one of their own, Emanuel Macron, a WEF Young Global Leader, to finally put a $number on the table. Macron offered Africa a billion dollars to finance vaccine production on the continent. It is not clear whether this is a loan or a grant, but it is clearly an initial step toward gaining favor for the Pandemic Treaty.
We will remain engaged as the treaty process develops.
What was really agreed to at the WHO on June 1, 2024?
https://merylnass.substack.com/p/complete-article-by-article-analysis
In order to explain the import of the IHR amendments that were adopted at the World Health Assembly on June 1, I have endeavored to compare the set of amendments proposed by the WHO in February 2023 with the amendments actually adopted on June 1, 2024. I hope this provides a detailed look at what the WHO hoped to obtain, and what it actually got: not much, considering its initial ask. But we must remain vigilant, as the people who captured the WHO won’t be packing up their toys and going home. Not yet, anyway. But we sure dodged the first cannonball they lobbed at us.
The WHO’s processes are sneaky and imho fraudulent, but no nations have cared enough to issue formal complaints. And they are the only ones with the power to make the WHO obey its own rules.
Here are the links to the WHO's initially proposed International Health Regulations (IHR) amendments of 6 February 2023 and what actually got passed (adopted) on June 1, 2024. Please remember that I am a doctor, not a lawyer, and these are my impressions. I will only comment on things I think are of particular relevance.
Here is something else there is confusion about: the adopted changes will not go into effect for 12 months for most countries and 24 months for others. So the version of the IHR that is in force currently is the (2005) version, which went into force in 2007. The bolding and crossed out words are the changes to this 2005 version. By paying attention to what is bolded and crossed out you can also see what the existing IHR (2005) looks like.
Above I screenshot both document titles so you can see which 2 documents I am comparing.
Below is the key for understanding the meaning of the bold language and struck through language described in the 6 February 2023 proposed amendments. 
Let me explain something else that has troubled people. They are concerned that the WHO Director-General (D-G) will be allowed to declare public health emergencies at will, after consultation. That is true, but in earlier versions, once the D-G made such a declaration, he had the power to order nations to do any number of things. In the adopted version of the IHR, he is not being granted those powers. So the declaration does not mean very much at this time.
Article 1 Definitions
Article 1 as proposed crossed out "non-binding" for both temporary and standing recommendations. This meant that all "recommendations" were to become binding "advice." In other words, they would no longer fit the meaning of recommendations or advice, and instead they would become orders. This was tricky language some lawyer for the WHO came up with, but it was almost immediately exposed. People did not like it.
In the adopted version, "non-binding" is no longer crossed out. This means that all recommendations and advice have returned to their clear meaning (recommendations only) and there is no requirement that nations comply with the "advice." This is extremely important because it removed the teeth from nearly every article in the rest of the document.
Article 2 Purpose and Scope
Article 2 as adopted got rid of the claim that the purpose of the IHR included "health systems readiness and resilience"–which is good, because the proposed terminology was very loose, and a lot of requirements for health systems could be snuck in later as being necessary for readiness or resilience.
The current (2005) version of the IHR noted that public health responses should be a) "commensurate with and restricted to public health risk" and b) "avoid unnecessary interference with international traffic and trade."
The proposed version expanded possible responses to a) "all risks with a potential to impact public health"– in other words, anything that might affect health, such as climate change, firearms, sugary drinks, or many other things.
The proposed version of b) was interesting. The meaning of the sentence was changed in the proposed version to avoid unnecessary interference with (language added:) livelihoods, human rights, and equitable access to health products and information. In other words, while such language did not fit well in a section on Scope and Purpose, it was placed there in order to sneak in the word "unnecessary." What the sentence then indicated is that it would be okay, when necessary, to interfere with livelihoods, human rights, and equitable access to health products and information. This was consistent with the crossing out of human rights in proposed Article 3, and therefore I believe the use of the word “unnecessary” was intentional. Who decides when it is “necessary”? This is a weasel word, providing a loophole enabling lockdowns, human rights abuses, restriction of medication and censorship.
All the worrying changes in the proposed IHR Article 2 that I just described were not included in the amendments that were adopted.
Article 3 Principles
The proposed Article 3, paragraph 1 attempted to fool readers by removing the existing IHR language, which guaranteed that implementation of the IHR must respect "dignity, human rights and fundamental freedoms of persons." These are rights that are specifically laid out in UN treaties and other documents. The proposal replaced this with language that did not have legal meaning and was ambiguous besides, while intended to convey an aura of "equity." The replacement language was: "based on the principles of equity, inclusivity, coherence."
The adopted Article 3 paragraph 1 amendment retained all the original language that guaranteed rights, while adding the words equity and solidarity: "The implementation of these Regulations shall be with full respect for the dignity, human rights and fundamental freedoms of persons, and shall promote equity and solidarity." No rights were lost, and equity and solidarity were added. Of interest, neither equity nor solidarity are defined in the extensive list of definitions in Article 1.
Paragraph 2 simply states an old fact: the IHR implementation should conform with the UN Charter and WHO Constitution. Just like US law must conform with the Constitution. I am not sure why people took issue with this.
Article 4 Responsible Authorities
There already exists a "National IHR Focal Point" in every nation whose role is to notify the WHO of possible outbreaks, etc. This is an old requirement.
Article 4 creates a second entity, the "National IHR Authority" in each nation, but allows nations to have one entity serving both roles. The role of the IHR Authority is to implement the IHR regulations. Note that in the proposed version, this entity would be "held accountable" for delivering IHR "obligations"–in other words, nations would be forced to comply with their "obligations." All this accountability/obligations language was removed from the adopted version of article 4.
Paragraph 2 is about getting information to the WHO in a speedy fashion, through the Focal Points and Contact Points. Since one of the main reasons to amend the IHR, according to the US, was to be sure that pandemics will not be hidden by national governments, it makes sense that the state parties demand details about how the information about possible outbreaks will be passed on and who will be responsible for doing so.
In paragraph 3 of the proposed article 4, nations were to be asked or required to pass legislation to give power and funding to the Focal Points. This language, reproduced below, is gone in the adopted IHR.
NEW (1bis) States Parties shall / ALT may enact or adapt legislation to provide National IHR Focal Points with the authority and resources to perform their functions, clearly defining the tasks and function of then entity with a role of National IHR Focal Point in implementing the obligations under these Regulations.
Article 5 Surveillance
This adopted article newly establishes the norm that nations will be expected to meet core capacities in their public health response within 5 years, or longer if an extension is granted. WHO is to assist developing nations meet this requirement, but it is not stated what WHO must do. Open-ended, more extensive requirements in the proposed version were not in the adopted version. One African nation (Uganda?) noted in its discussion after the new IHR was adopted that it has small outbreaks all the time and it would be onerous and unrealistic to require early reporting of all of them. This statement portends that African nations may issue reservations or rejection of the surveillance and notification provisions of the adopted IHR. They have 10 months (or for a few nations, 18 months) to do so.
Article 6 Notification
The proposed Article 6 wanted very specific genetic sequencing data, specimens, and detailed epidemiological information to be transferred from nations with an outbreak to the WHO. The WHO would then share this information with all Parties. This was not adopted.
The proposed version then stated (disingenuously):
" WHO shall not transfer the public health information received…[to entities] engaging directly or indirectly with conflict and violence elements."
I found this proposal horrifying: WHO planned to share pandemic pathogens with anyone who wanted them, with the exception of those "engaging… with conflict or violence elements"?
Why did WHO plan to proliferate microorganisms that could cause pandemics? The WHO's use of this language seemed to me to be an attempt to obtain tacit agreement from nation states for the act of proliferation.
The adopted Article 6 fails to say anything about the WHO transferring materials. It omits the terms "genetic sequence data" and while it requires information, it is much less specific about what information nations must provide.
Article 7 Information-sharing during unexpected or unusual public health events
The proposed language demanded that nations supply microbial samples and genetic sequence data to WHO. The adopted language simply says nations will supply all relevant public health information. I was struck by how aggressively the WHO demanded genetic sequence data in many versions of the documents and was pleased that such language was removed everywhere.
Article 8 Consultation
Not much of significance changed
Article 9 Other Reports
The proposed article removed the requirement that the WHO would have to consult with the nation in whose territory an outbreak was occurring before taking action. This was not removed in the adopted version.
This wording was proposed:
(New wording) "In the recommendations made to the States Parties regarding the collection, processing and dissemination of health information, WHO could advise the following: (a) To follow the WHO guidelines on criteria and analogous modes of processing and treating health information."
Remember that in the proposed version, 'advise' could mean "order' (if the term 'non-binding' had been eliminated as proposed, which did not make it to the adopted version). This would have given WHO wide berth regarding what information WHO demanded from nation states and what WHO could do with the information.
Article 10 Notification
Insignificant
Article 11 Provision of information by WHO
Insignificant
Article 12 Determination of a public health emergency of international concern, including a pandemic emergency
The proposed amendment included more than a page of language about emergencies that were not severe enough to meet a PHEIC, or were regional emergencies or potential emergencies. This language was removed from the adopted version. There is no option for declaring "potential" emergencies as was desired.
Article 13 Public health response, including equitable access to relevant health products
The WHO is to assist nations to obtain or produce health products, but there are no real specifics or guarantees of what assistance will be provided. Product dossiers will be shared if manufacturers agree. This is what developing nations wanted but they got nothing concrete.
Article 14 Cooperation of WHO with intergovernmental organizations and international bodies
No change
Article 15 Temporary recommendations
The proposed article included "The recommendations based on these assessments shall include:
(a) support by way of epidemic intelligence surveillance, laboratory support, rapid deployment of expert teams, medical countermeasures, finance as well as other requisite health measures to be implemented by the State Party experiencing the Public Health Emergency of International Concern"
You may remember a video of bill Gates discussing the deployment of expert teams flying to an outbreak to gather information and maybe perform other tasks. The 2023 NDAA also talks about the US sending "teams" [military] to foreign nations when the USG is not being given sufficient information about an outbreak. The CDC has long sent epidemic intelligence service staff to outbreaks on request, but the language used here could have opened the door to CDC and its quasi-military Public Health Service members entering uninvited.
I don't think most nations want the US or anyone else barging in to "assist" without being invited. The word "shall" in a treaty means "must," and that, along with the original plan to make these articles binding, would have made every nation susceptible to being invaded by foreign teams in response to suspected outbreaks. The adopted version did not include any of this.
Article 16 Standing recommendations
Insignificant
Article 17 Criteria for recommendations
Insignificant
Article 18 Recommendations with respect to persons, baggage, cargo, containers, conveyances, goods and postal parcels
The proposed article included this:
"ensure mechanisms to develop and apply a traveller's health declaration in international about travel itinerary, possible symptoms that could be manifested or any prevention measures that have been complied with such as facilitation of contact tracing, if necessary…"
This was not included in what was adopted. Other changes are insignificant. So contact tracing was removed.
People are confused by article 18 because as proposed, recommendations would have become orders and therefore it was going to give the Director-General the right to order lockdowns, vaccine mandates, quarantines, etc. But since the word non-binding was not crossed out, recommendations remain recommendations. So the Director-General cannot order any of these things.
Article 19 General obligations
Insignificant
Articles 20-22 were essentially unchanged
Article 23 Health measures on arrival and departure
This is where health documents and "passenger locator forms" which could be used for contact tracing were to be enforced in the proposed IHR. But the old IHR was retained (adopted) without changes.
Article 24 Conveyance operators
The proposed article added the ability for conveyance operators to "implement quarantine promptly on board as necessary." This was dropped in the adopted IHR. See article 27. Only a competent authority can quarantine a ship or plane – so the US would not be the competent authority, presumably, and therefore it would not be legally able to quarantine another Diamond Princess when it is located in a foreign country.
Articles 25 and 26 are unchanged
Article 27 Affected conveyances
The ability for a "competent authority" to quarantine a conveyance was adopted.
Articles 28-34
No changes
Article 35 General rule
Authentic paper or digital health documents are required, but the proposed need for a QR code and detailed language on authenticity is gone.
Articles 36-42 are essentially unchanged
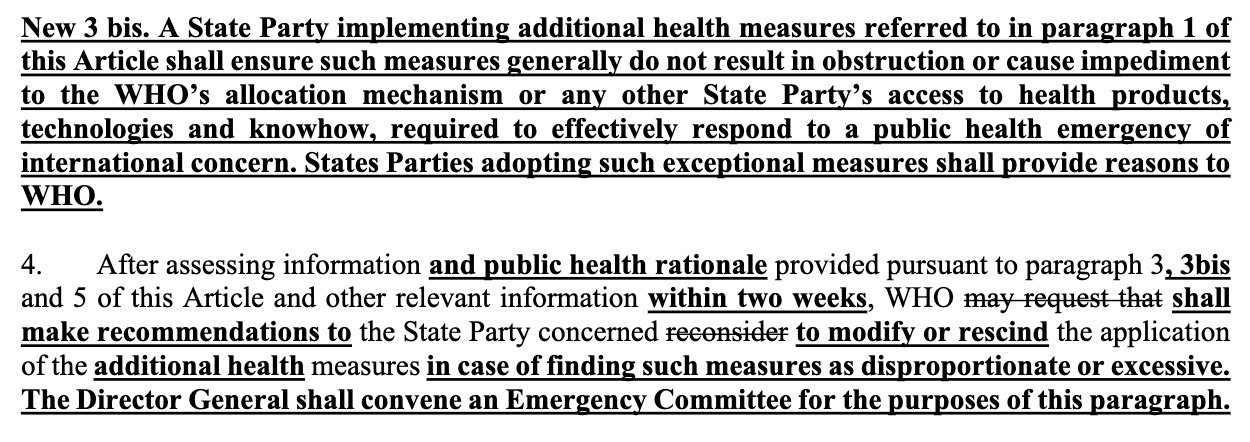
Article 43 Additional health measures
The proposed article 43 paragraphs New 3 bis. and 4 used tricky language to give the WHO Director-General the right to withhold medications if he found them to be "disproportionate or excessive." This was the unbelievably bad clause to be used to stop people obtaining hydroxychloroquine, ivermectin, vitamins or other substances during declared emergencies. The adopted article 43 did not include this.
Article 44 Collaboration and assistance and Article 44 bis.
The proposed article established a funding mechanism for the IHR to provide assistance to developing countries to meet the obligations they would take on for pandemic preparedness activities, including core capacities. A funding mechanism for pandemic preparedness has already been established in 2022 jointly through the WHO and World Bank but is funded with under $2 Billion. Estimates are that the pandemic program envisioned by the WHO would cost $30-42 Billion/year.
The obligations for which funding might be provided, or loaned, would have included:
"1. (c) (New) building capacity to identify emerging public health threats, including through laboratory methods and genome sequencing; (c) (new) strengthening capacity to identify health threats including through surveillance, research and development cooperation, technological and information sharing. (e) (new) collaborating with each other, with WHO, the medical and scientific community, laboratory and surveillance networks, to facilitate timely, safe, transparent and rapid exchange of specimens and generic sequence data for pathogens with the potential to cause pandemics and epidemics or other high-risk situations… digital technologies to improve and modernize communication for preparedness and response to health emergencies, including to better meet the obligations of these Rules (h) (new)in countering the dissemination of false and unreliable information about public health events, preventive and anti-epidemic measures and activities in the media, social networks and other ways of disseminating such information"
This language above, listing expectations c) — h) is missing from the adopted version.
I anticipate that nations will be given small grants while being encouraged to take on large debt obligations to meet their "core capacities" and potentially build out other parts of the pandemic preparedness agenda.
Articles 45-47 are unchanged
Article 48-53 had only minor changes
Article 54 and 54 bis.
The adopted version does establish an implementation committee though it omits the proposed compliance committee. The proposed IHR suggested it wanted to be able to have enforcement powers. In the adopted version, the implementation committee is specifically stated to be advisory only:
1. The States Parties Committee for the Implementation of the International HealthRegulations (2005) is hereby established to facilitate the effective implementation of these Regulations, in particular of Article 44 and 44bis. The Committee shall be facilitative and consultative in nature only, and function in a non-adversarial, non-punitive, assistive and transparent manner, guided by the principles set out in Article 3.
Articles 55-66 are unchanged
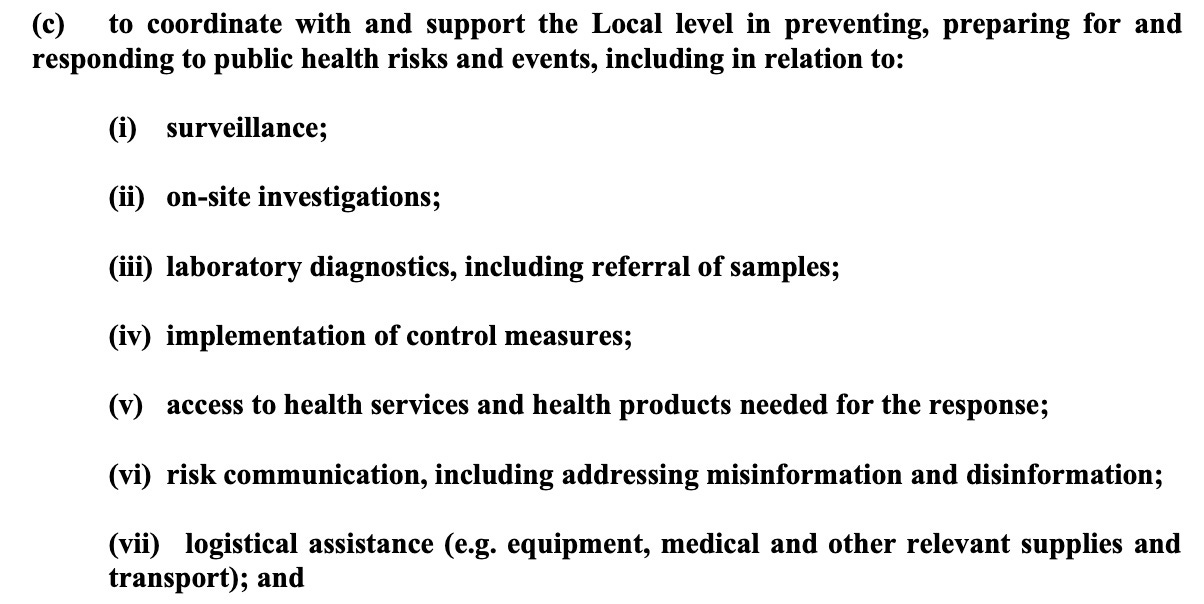
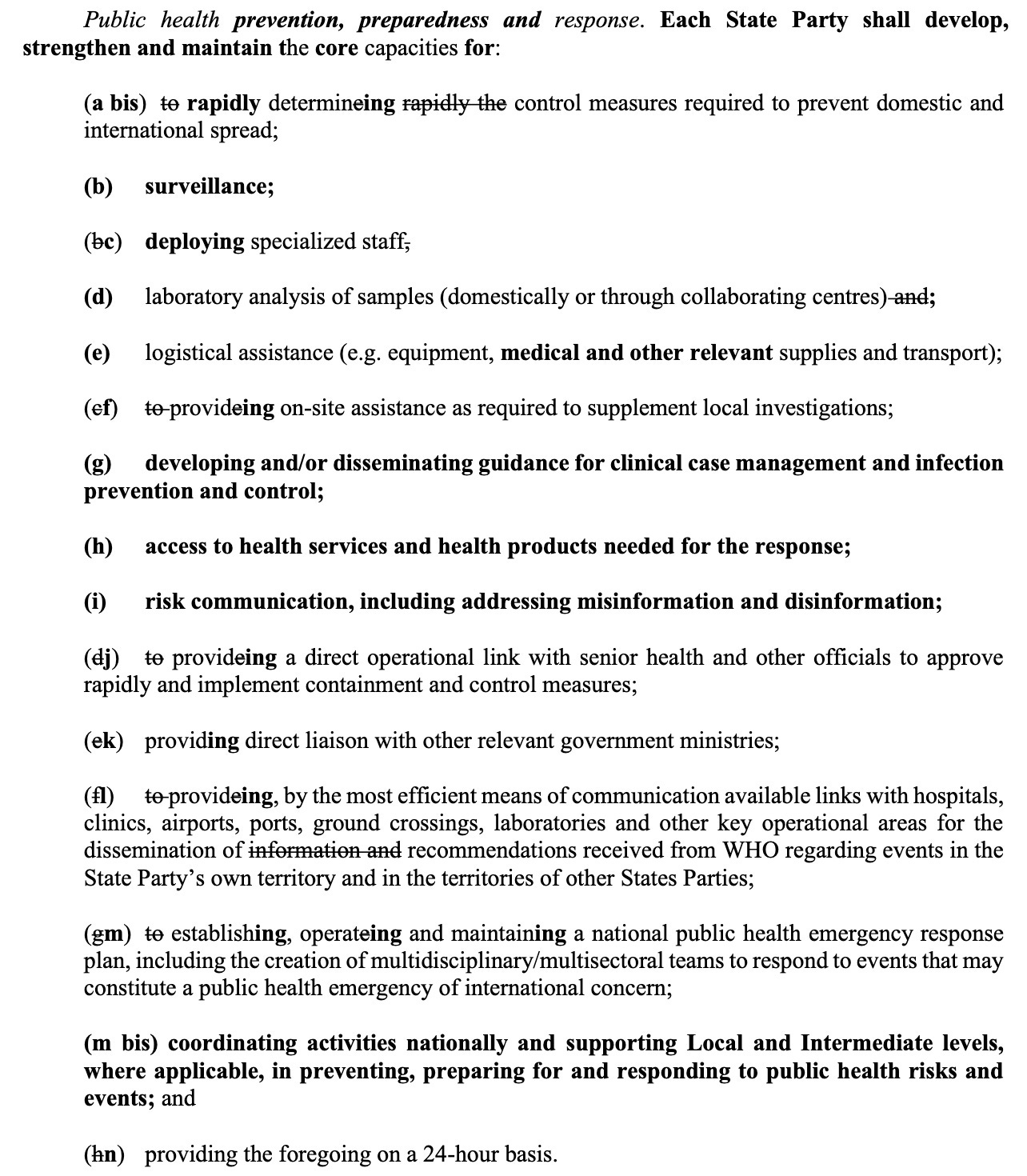
ANNEX 1. A Core Capacities
Countries will be obliged to take on new obligations in this ANNEX, and surveillance and censorhip are among them, both at the national and local levels.
This is where we lost, but I was expecting to lose this because, as other items were jettisoned in successive drafts, this obligation always remained. And all Western nations and probably most others as well are already surveilling and censoring their citizens:
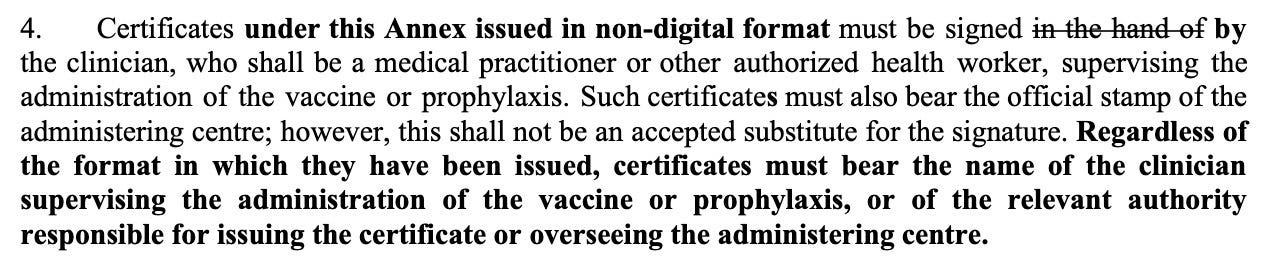
ANNEX 6. VACCINATION, PROPHYLAXIS AND RELATED CERTIFICATES
This is the section where the language is loose enough for people to obtain "fake" vaccine certificates. There is no requirement for "true" authentication. No need for a QR code. The authorities are essentially requiring the same level of authentication required when I went to Africa in 1972, rather than detailed authentication that was proposed. The nations would not agree to tighten the health certificate rules so that it would be extremely difficult to avoid being vaccinated. They wanted a way out.
Hoping this helps you understand the battle we waged for the past two years.